
With an understanding of the definition of critical care from Part 1 of this series, What Constitutes Critical Care?, below are essential documentation and coding guidelines for Emergency Management physicians to ensure they receive the reimbursement they deserve.
Critical care is a time-based service and must be documented as the time the provider spent evaluating, providing care and managing the critically ill or injured patient. It may be continuous or intermittent and aggregated, but time must always be documented precisely in minute increments.
Time spent with family members or other decision makers, whether to obtain history or to discuss treatment options, may be counted toward critical care time when these specific criteria are met:
-
The patient is unable or incompetent to participate in giving a history or making treatment decisions and
-
The discussion is necessary for determining treatment; this necessity must be documented.
Time spent reviewing laboratory test results or discussing the critically ill patient’s care with other medical staff may also be reported as critical care if this activity requires the physician’s full attention.
Time spent in activities that occur outside of the unit or off of the floor (e.g., telephone calls taken at home, in the office or elsewhere in the hospital) cannot be counted as critical care because the physician is not immediately available to the patient.
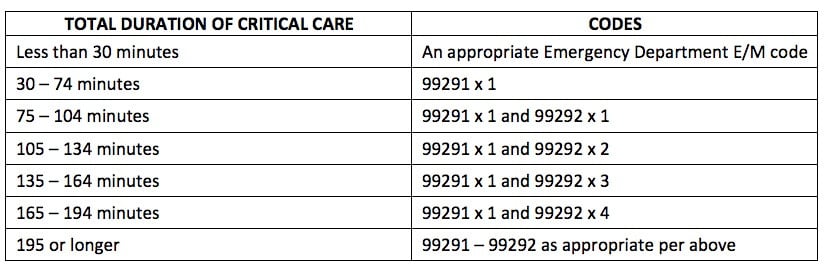
Critical care codes are based on the total duration of care, outlined in the table below:
-
Critical care time of less than 30 minutes is coded with an appropriate Emergency Department E/M code.
-
Only one unit of CPT code 99291 may be billed by a physician for a patient on a given date.
-
Critical care documentation must reflect an exact number of minutes. For example, a physician would document 38 minutes, not a range (e.g., 30-74), as reflected in the documentation of critical care time in a chart.
-
The following services are included in critical care and cannot be billed separately when performed by the same provider during the critical care time: Interpretation of cardiac output measurements, chest x-rays, pulse oximetry, blood gases and collection and interpretation of physiologic data, gastric intubation, temporary transcutaneous pacing, ventilatory management and vascular access procedures.
-
Critical care time reported must exclude time spent on other billable procedures; for example, CPR, central line placement and intubation.
-
The initial critical care time of 30 minutes, billed as CPT code 99291, must be met by a single physician or NPP; this may be performed in a single period of time or be aggregated by the same provider on the same calendar date.
-
Subsequent critical care visits performed for the same patient on the same date of service are reported using CPT code 99292. The service may represent aggregate time met by a single physician or physicians in the same group practice with the same medical specialty in order to meet the duration of minutes required for CPT code 99292. The aggregated medical care visits must be meet the definition of critical care, and be documented, in order to combine the times.
-
Physicians of the same specialty within the same group practice bill and are paid as though they were a single physician and cannot each report CPT code 99291 for a patient on the same day of service.
-
A split or shared service performed by a physician and a qualified Non-Physician Provider (NPP) of the same group practice or employer cannot be reported as a critical care service.
-
The codes above are used for all patients who are critically ill or injured over the age of 5 years old; if the patient is under 5, the neonatal or pediatric critical care codes are reported.
Emergency Medicine physicians must be highly educated, trained and skilled to provide critical care for patients with life-threatening injuries and illnesses. By following the critical care documentation and coding guidelines outlined above, physicians can help to ensure that they receive the compensation they deserve for their extraordinary work.